Unilateral perisylvian syndrome- Typical presentation of a rare entity.
DESCRIPTION
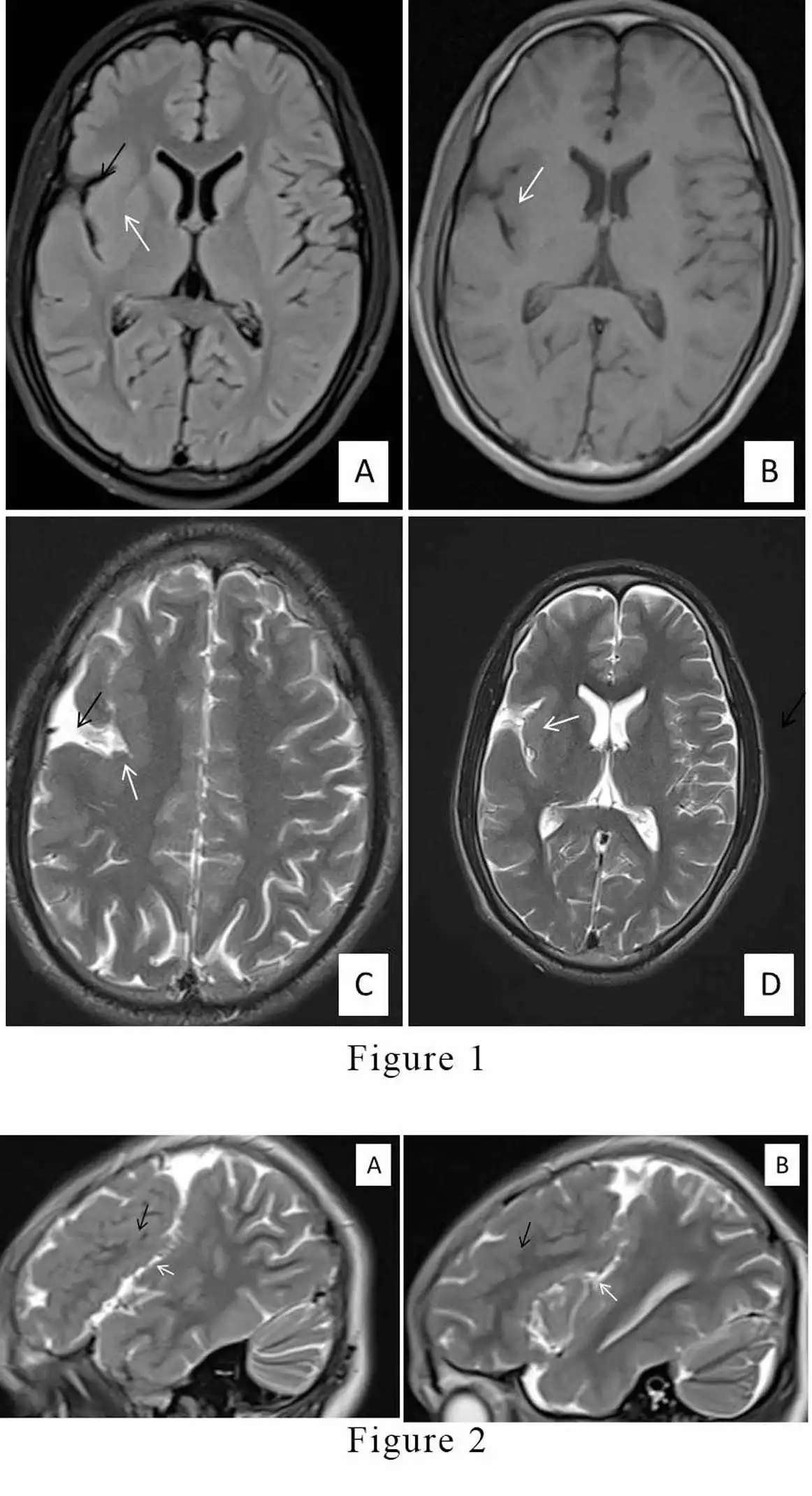
Congenital perisylvian syndrome or perisylvian polymicrogyria is a malformation of abnormal migration of neurons during intra-natal period.[1] It affects the areas in the cerebral cortex surrounding Sylvian fissures and peri-insular circular sulcus. Although the exact timing and mechanism are unclear, assumptions are made that this neural dysmigration is estimated to occur before 30 weeks of gestation. It is a neurological disorder that has typical radiological findings related to polymicrogyria.[2,3,4] This entity usually affects bilateral side of cortex. Unilateral polymicrogyria is a rare subtype, which is present in our case.Symptomatically, the patients present with upper motor neuron clinical features such as pseudobulbar palsies, dysarthria, dysphagia, and tongue weakness since it affects the of cortico-bulbar tract. These patients may have seizures, and delayed language, and motor milestones; however, dysarthria is a relatively common feature. [2,4] that can range from mild impairment to anarthria. Magnetic resonance imaging (MRI) of the brain is the imaging modality of choice for its diagnosis. MRI findings have revealed that explicitly perisylvian cortical polymicrogyria, characterized by multiple abnormally formed small convolutions with shallow sulci. The Sylvian fissures are wide and underdeveloped, and the opercula are dysplastic and incomplete. MRI has also helped in grading the severity of the disorder (Grade 1 is the most serious type and Grade 4 is the mildest one). Grade 1 is described as perisylvian microgyria extending to the frontal or occipital pole; Grade 2 comprises polymicrogyria that expands beyond the perisylvian region but not reaching the pole; Grade 3 includes polymicrogyria of the perisylvian region only, and Grade 4 is polymicrogyria restricted to posterior perisylvian regions only.[4] The treatment and therapies aim to treat or improve the signs and symptoms of the patient. Symptomatic treatment includes antiepileptic and multiple rehabilitative measures like speech therapy, training in oral motor skills in swallowing and tongue muscle exercises. A 14-year-old female patient presented to our hospital with complaints of difficulty speaking, trouble remembering things, and delayed milestones. She was having difficulty articulating speech; however, she was otherwise rhetorically normal (dysarthria) for the last three years. She also had a history of episodes of brief failure in awareness ( known as atypical absence seizures). Her birth and family history was unremarkable, and the patient did not have any dysmorphic phenotypic features. Neurological examination revealed a cognitive deficit with severe dysarthria along with restriction of tongue movements. MRI of the brain revealed abnormal cortical thickening involving the right perisylvian cortex.[Figue 1A,1B,1C,1D & 2A,2B]. Moreover, poor delineation of grey-white matter architecture was observed in this region, along with abnormal sulcation and numerous closely spaced abnormal gyri (polymicrogyria). The MRI also illustrated the widening of the right sylvian fissure.[Figue 1A,1B,1C,1D & 2A,2B] The cortical thickness in the perisylvian region was measured up to 12 mm. The clinical features and typical imaging findings suggested the diagnosis of congenital unilateral perisylvian syndrome. The parents were confabbed about the disease, and the child was given a tutorial for oral motor skills and speech therapy. The patient is gradually improving symptomatically till the last hospital visit.
LEARNING POINTS
-
MRI is the best modality for paediatric patients presenting with neurological disorder for making an early diagnosis and to start appropriate treatment timely.
-
Unilateral perisylvian syndrome is the rarest developmental malformation of the brain which do not have any definite cure at presnt, only symptomatic treatment is the main stay along with the rehabilitaion therapy.
LEGENDS:
-
Barkovich AJ, Kuzniecky RI, Jackson GD, Guerrini R, Dobyns WB (2005) A developmental and genetic classification for malformations of cortical development. Neurology 65:1873–1887
-
Kuzniecky R, Andermann F. The congenital bilateral perisylvian syndrome: Imaging findings in a multicenter study. CBPS Study Group. AJNR Am J Neuroradiol 1994;15:139-44.
-
Taneja S, Chaturvedi A. Bilateral perisylvian syndrome- A case report. Indian J Radiol Imaging 2006;16:169-71.
-
Barkovich AJ. Current concepts of polymicrogyria. Neuroradiology 2010;52:479-87
FIGURE CAPTIONS
-
Figure 1: Magnetic resonance images (MRI) A) Flair sequence, B) T1 sequence C), D) T2 sequence axial plane images depicting widened right Sylvian fissures (Black arrows) and thickening of right perisylvian cortex (of the right frontal and temporal lobes) (White arrows) with polymicrogyria.
-
Figure 2: Magnetic resonance images (MRI) T2 sequence sagittal plane images shows widened right Sylvian fissures (White arrows) and right perisylvian thickened cortex ( Black arrows).