Pituitary apoplexy- A potentially fatal condition
DESCRIPTION
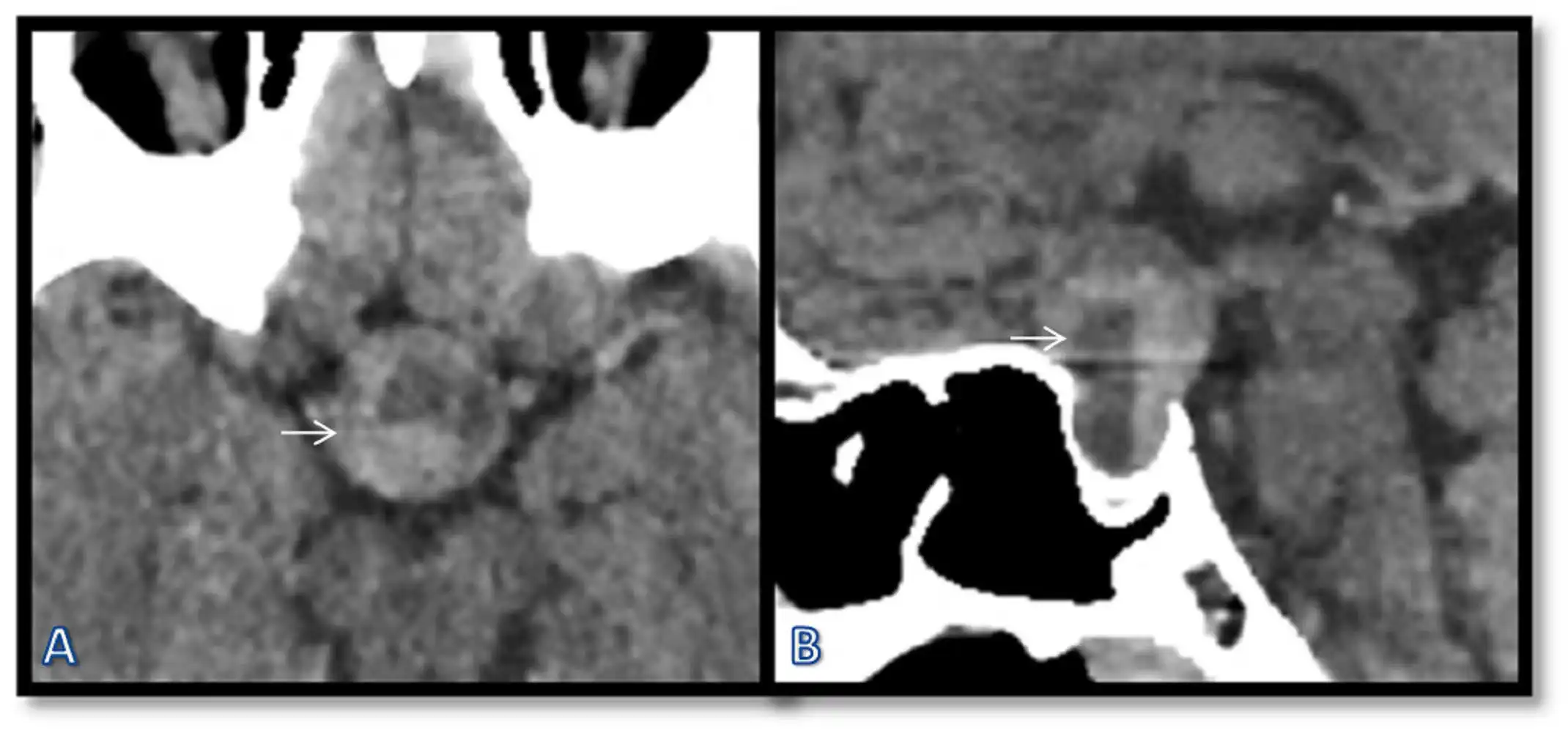
Pituitary apoplexy is an unusual condition that is often fatal. It has a male predisposition and a mean age of onset around 57 years.[1] It usually occurs in patients with pre-existing pituitary mass lesion like macroadenoma, which undergoes a hemorrhagic infarction in the lesion. The patient presents with acute headache, visual impairment, altered mental status, vomiting and panhypopituitarism.[2,3,4] The patient may directly present with the complications without being previously diagnosed with macroadenoma. The most common presentation is sudden onset headache, mainly retro-orbital, which may be confused with thunderclap headache. This presentation may make the clinician suspect SAH.[5] The second most common presenting feature is a visual deficit, followed by vomiting, nausea, and neurological deficits. The computerised tomography (CT) of the head usually shows sellar enlargement with an expansile pituitary lesion. There are areas of patchy or confluent hyperdensities within the lesion. There may also be layering in the lesion, possibly due to different densities of blood products. The patient may have a haemorrhage in the adenoma without being symptomatic; in such conditions, the term pituitary apoplexy is not used. A 49-year old female presented with a severe headache. She was previously diagnosed with pituitary macroadenoma, for which she did not take any treatment. She was advised unenhanced CT scan of the head. A large well-defined oval-shaped lesion was seen in the pituitary gland with internal areas of haemorrhage forming blood-fluid levels [white arrow in Figure 1(A) & (B)].
LEARNING POINTS/TAKE HOME MESSAGES
-
Pituitary apoplexy is mostly a complication of patients with pre-existing macroadenoma.
-
Headache, visual impairment, vomiting, altered mental status are the common presenting symptoms of pituitary apoplexy.
-
CT is the first investigation done in suspected pituitary apoplexy, which will reveal internal haemorrhage.
REFERENCES
-
Dubuisson AS, Beckers A, Stevenaert A. Classical pituitary tumour apoplexy: clinical features, management and outcomes in a series of 24 patients. Clin Neurol Neurosurg. 2007;109:63–70. doi: 10.1016/j.clineuro.2006.01.006. [PubMed] [CrossRef] [Google Scholar].
-
Brougham M, Heusner AP, Adams RD. Acute degenerative changes in adenomas of the pituitary body—with special reference to pituitary apoplexy. J Neurosurg. 1950;7:421–439. doi: 10.3171/jns.1950.7.5.0421. [PubMed] [CrossRef] [Google Scholar]
-
Wakai S, Fukushima T, Teramoto A, Sano K. Pituitary apoplexy: its incidence and clinical significance. J Neurosurg. 1981;55:187–193. doi: 10.3171/jns.1981.55.2.0187. [PubMed] [CrossRef] [Google Scholar]
-
Cardoso ER, Peterson EW. Pituitary apoplexy: a review. Neurosurgery. 1984;14:363–373. doi: 10.1227/00006123-198403000-00021. [PubMed] [CrossRef] [Google Scholar]
-
21. Schwedt T, Matharu M, Dodick D. Thunderclap headache. Lancet Neurol. 2006;5:621–631. doi: 10.1016/S1474-4422(06)70497-5. [PubMed] [CrossRef] [Google Scholar]
INTELLECTUAL PROPERTY RIGHTS ASSIGNMENT OR LICENCE STATEMENT
I, Dr. Rajaram Sharma, the Author has the right to grant and does grant on behalf of all authors, an exclusive licence and/or a non-exclusive licence for contributions from authors who are: i) UK Crown employees; ii) where BMJ has agreed a CC-BY licence shall apply, and/or iii) in accordance with the relevant stated licence terms for US Federal Government Employees acting in the course of the their employment, on a worldwide basis to the BMJ Publishing Group Ltd (“BMJ”) and its licensees, to permit this Work (as defined in the below licence), if accepted, to be published in BMJ Case Reports and any other BMJ products and to exploit all rights, as set out in our licence author licence.