Contrast CT evaluation of an isolated renal hydatid cyst.
DESCRIPTION
Hydatid disease is a zoonotic disease caused by Echinococcus granulosus or Echinococcus multilocularis.[1] Rudolph, in 1808 first used the term “hydatid” to describe echinococcosis,which in ‘Greek’ means watery vesicle. Definitive hosts of the disease are dogs, foxes, or other canids.[2] Humans are accidental hosts of the disease in whom it can affect almost every system.[3] Urinary tracts are the rarely involved organ in this entity, and secluded renal involvement is rare (2–4% of all cases).[4,5] The patient usually presents with non-specific symptoms like hematuria, vague flank or lower abdominal pain, or it may rupture, leading to hydatiduria. Renal hydatid cysts are classified into five types, (a) Type I cysts are unilocular, without internal architecture, (b) Type II cysts contain focal or diffuse detachment of the inner germinal layer, (c) Type III cysts are multiseptated daughter cysts,(d) Type IV which contain dense folded membranes, internal echoes and has the heterogeneous appearance, and (e) Type V has pericystic ring-like calcification, signifies dead parasite.[6] It can mimic other renal pathologies due to its morphological resemblance; however, the combinations of characteristic imaging findings and serological tests (like hypereosinophilia) usually make the diagnosis.Ultrasonography (US) and computed tomography (CT) are commonly used imaging modalities; however, most of the time, a CT scan is needed to exclude close differentials like a simple cortical cyst, abscess, cystic nephroma. The cyst wall in type I hydatid cyst and the daughter cysts of type II are better delineated with contrast-enhanced CT than sonography. Contrast CT imaging also helps differentiate abscess, as an abscess will show a thick enhancing wall, internal necrosis, thickening of Gerota's fascia, and perirenal fat stranding. The CT scans also help differentiate between Type IV hydatid cysts and tumours, as the CT can easily demonstrate multiple daughter cysts and delineate ring-like calcification along the cyst wall, which signifies a hydatid cyst while avid heterogeneous enhancement in the lesion favours a neoplastic lesion. The CT scan can also assess the other viscera at one go. Surgery is the mainstay treatment for symptomatic renal hydatid cyst through open access or the retroperitoneal approach; however, the retroperitoneal approach is preferred to avoid contamination or spread.[7] A 45 years old female came to our surgery department with a complaint of pain in the right flank region. On physical examination, she had mild fullness in her right lumbar region; however, rigidity/tenderness was present. The routine blood investigations were normal. For further assessment, she underwent a US scan of the abdomen, which demonstrated a complex heteroechoic multicystic lesion in the mid-lower pole of the right kidney. After that, a contrastenhanced computed tomography (CECT) scan of the abdomen was performed, which revealed a thick-walled cystic lesion with multiple daughter cysts. It had ring-like calcifications along the walls of the daughter cysts, and it did not enhance on post-contrast phases.[Figure 1A,1B,1C & 1D] A final diagnosis of renal hydatid cyst was made. The post-operative period was uneventful and patient was on follow up.
LEARNING POINTS
A renal hydatid cyst is an infrequent entity. Isolated renal hydatid cyst can easily be misdiagnosed. Therefore a thorough radiological investigation is essential, and CECT is the modality of choice for that.
LEGENDS:
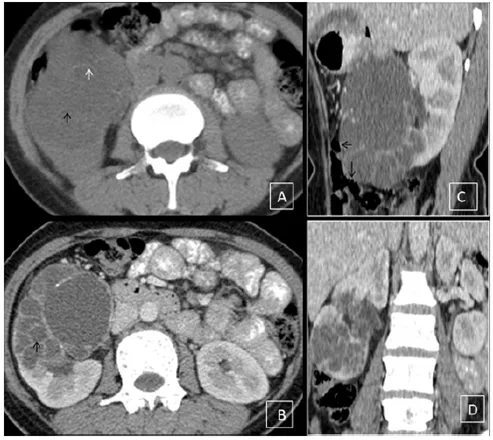
Figure 1: Computed tomography scan of the abdomen (A) Non-contrast axial plane image illustrate a well defined cystic lesion with thin internal septations involving the middle and lower pole of the right kidney (black arrow) with peripherally placed ring-like calcification (white arrow). (B) Post-contrast axial plane images illustrate multiloculated cystic lesions with internal daughter cysts (black arrow). Post-contrast computed abdominal tomography scan (C) Sagittal plane (D) Coronal plane images demonstrate large cyst with a non-enhancing wall (black arrow) and internal septations involving middle and lower pole of the right kidney.
REFERENCES
-
Mowlavi G, Kacki S, Dupouy-Camet J, Mobedi I, Makki M, Harandi MF, Naddaf SR. Probable hepatic capillaries and hydatidosis in an adolescent from the late Roman period buried in Amiens (France). Parasite 2014; 21: 9 [PMID: 24572211].
-
J. Eckert and P. Deplazes, “Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern," Clinical Microbiology Reviews, vol. 17, no. 1, pp. 107– 135, 2004.
-
JH. Akkaya, B. Akkaya, and S. Gon¨ ulc ¨ u, “Hydatid disease ¨ involving some rare sites in the body,” TurkiyeParazitolojii ¨ Dergisi, vol. 39, no. 1, pp. 78–82, 2015.
-
R. Garg, U. Nahar, and A. K. Mandal, “A rare case of primary renal hydatid cyst,” Annals of Parasitology, vol. 61, no. 2, pp. 129– 131, 2015
-
S. A. Kumar, A. Shetty, C. Vijaya, and V. Geethamani, “Isolated primary renal echinococcosis: a rare entity,” International Urology and Nephrology, vol. 45, no. 3, pp. 613–616, 2013.
-
Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. RadioGraphics 2003; 23:475–49
-
M. M. Agarwal and A. K. Hemal, “Surgical management of renal cystic disease,” CurrentUrology Reports, vol. 12, no. 1, pp. 3–10, 2011.